
There is a well-known Chinese idiom: “carving a mark on a moving boat to retrieve a lost sword.”
A man drops his sword into a river and calmly marks the position on the boat, believing he can retrieve it later from the same spot. What he fails to recognize is simple:
The boat has moved.
In many ways, this story has stayed with me when thinking about varicose vein treatment.
Over the past decades, our field has made remarkable progress. Technologies have evolved rapidly—procedures have become less invasive, more efficient, and more accessible to patients. These advances have undoubtedly improved care.
At the same time, the way we define the problem has been relatively consistent. When reflux is identified, the typical response is to address the vein directly, often by closing or removing it.
This approach has been effective in many situations.
But it may not capture the full picture.
Varicose veins are not only structural findings. They reflect a dynamic system—one shaped by pressure, flow, and the body’s continuous adaptation.
What we see on imaging is a moment in time.
What the system does, however, continues to evolve.
In a similar way, our understanding of iliac vein compression may also be influenced by how and when we observe it.
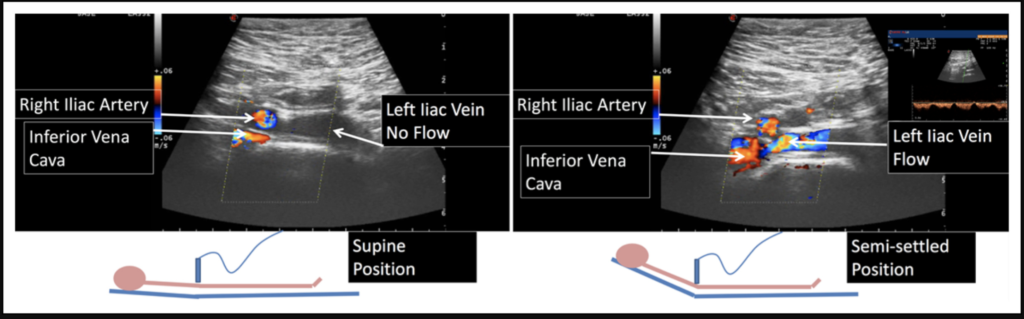
Most imaging studies—CT or MR venography—are performed with the patient in a supine position. What we see, therefore, reflects a single moment under specific conditions.
However, venous physiology is dynamic. When patients are upright or sitting, the relationship between anatomical structures and venous flow may change. In some cases, the degree of compression appears less pronounced, or functionally less significant.
This does not diminish the importance of identifying true outflow obstruction.
But it does remind us to interpret imaging findings within a broader physiological context.
By doing so, we may be able to better distinguish between anatomical compression and clinically relevant hemodynamic disturbance—and, in selected cases, avoid unnecessary interventions.

This is where I find myself returning to that simple story.
Rather than asking only which vein to treat, we begin to ask how the flow behaves, and how it might be guided. The objective shifts slightly—from removing a structure to understanding its role within the system.
Within platforms such as the Asian Venous Academy, there is a growing effort to bring together clinicians, engineers, and researchers—to rethink the foundations on which they are built.
There is a temptation in any field to refine the instrument— to make the blade sharper, more precise, more elegant.
But sometimes, the question is not how to perfect the tool,
but whether we are using it to solve the right problem.
Because no matter how refined the mark we carve,
it will not help us find the sword if the boat as already moved.



{kind=link}