
The treatment of Small Saphenous Vein (SSV) reflux presents a unique set of anatomical challenges that differ significantly from the Great Saphenous Vein (GSV). While endovenous thermal ablation (EVA) has become a common standard, clinical evidence and anatomical logic increasingly suggest that CHIVA (Cure Conservatrice et Hémodynamique de l’Insufficiency Veineuse en Ambulatoire) offers a superior safety profile—particularly regarding the prevention of nerve damage.
The Anatomical “Danger Zone”
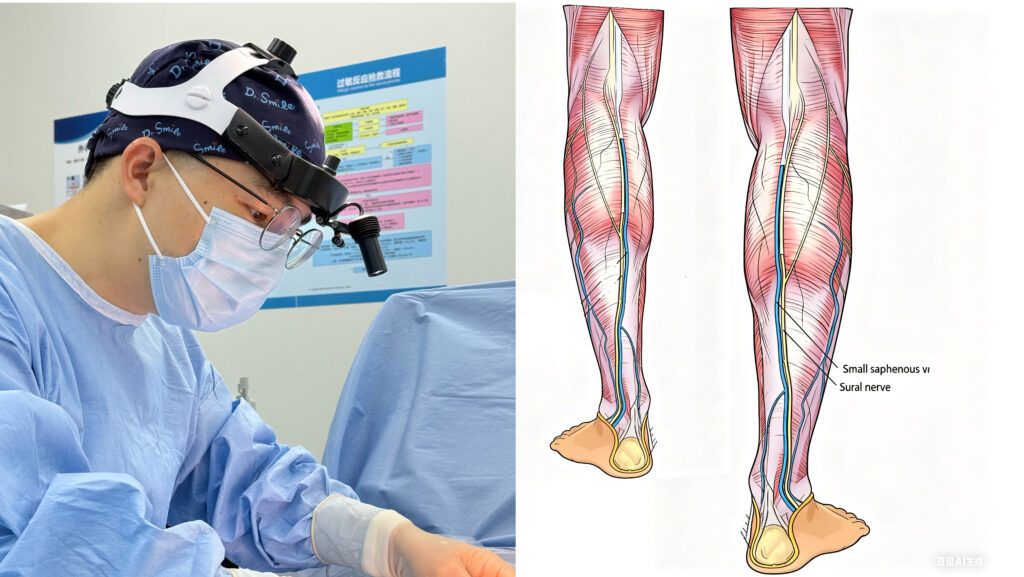
The primary concern during any intervention on the SSV is its intimate relationship with the Sural Nerve (SN) and the Tibial Nerve (TN).
In the distal two-thirds of the lower leg, the Sural Nerve and the SSV are nearly inseparable, often traveling within millimeters of each other. Unlike other regions where the deep fascia acts as a protective barrier, the distal SSV and Sural Nerve often share the same anatomical compartment without a fascial shield.
The Thermal Risk: Why Ablation Falls Short
Thermal ablation (laser or radiofrequency) relies on high temperatures to seal the vein. Even with the use of tumescent anesthesia as a heat sink, the “small distance” and “absence of deep fascia” in the distal leg make the Sural Nerve highly vulnerable to heat conduction.
Clinical studies indicate that nerve injury rates in SSV ablation can be significantly higher than in GSV procedures. This often results in:
- Paresthesia: Numbness or tingling along the outer foot.
- Chronic Pain: A persistent “burning” or “acid-aching” sensation.
- Hyperesthesia: Extreme sensitivity to touch.
The CHIVA Advantage: Hemodynamics Over Heat
CHIVA fundamentally changes the treatment paradigm. Rather than destroying the vein with heat, CHIVA uses precise, ultrasound-guided ligation to redirect blood flow from the superficial system back into the deep veins.
1. No Thermal Energy, No Nerve Damage Because CHIVA is a non-thermal, hemodynamics-based procedure, the risk of heat-induced injury to the Sural or Tibial nerves is mathematically zero. We do not “cook” the vessel; we simply “re-route” the traffic.
2. Preservation of the Fascial Barrier In the proximal third of the leg, the deep fascia acts as a natural barrier between the SSV and the Sural Nerve. CHIVA leverages this anatomical “safe zone” for its strategic ligations, ensuring that the intervention remains minimally invasive and biologically respectful.
3. Relief of “Nerve-Induced” Aching Many patients with SSV reflux suffer from a specific type of acid-aching or cramping. This is often caused by the high transmural pressure of the refluxing vein physically compressing the Sural Nerve. By instantly lowering the venous pressure through hemodynamic diversion, CHIVA often provides faster relief of these neurological symptoms than destructive methods.
The Surgeon Behind the Strategy: Why Experience Matters
The safety of CHIVA in treating Small Saphenous Vein reflux is not merely a result of the technique itself, but a reflection of the surgeon’s mastery over three critical pillars: Local Anesthesia, Ultrasound Precision, and Deep Anatomical Insight.
1. The Lost Art of Anatomy
In the era of “One-size-fits-all” thermal ablation, many practitioners have become overly reliant on the catheter, gradually losing touch with the intricate surgical anatomy of the popliteal fossa and the distal leg. Ablation is often performed as a “blind” thermal strike within the vessel.
In contrast, a CHIVA surgeon must be an expert in both hemodynamics and open dissection. We do not just see a “vein to be closed”; we see a complex map of nerves, fascia, and variable tributaries. This “Anatomical Memory” is the ultimate safety net for the patient.
2. Local Anesthesia as a Safety Monitor
We perform CHIVA under strict local anesthesia. This is not just for faster recovery; it is a deliberate safety choice. Unlike general anesthesia, local anesthesia allows for real-time patient bio-feedback. If a surgical maneuver nears a nerve, the patient’s sensory response acts as an immediate “alarm,” allowing us to adjust with a level of precision that thermal or general-anesthesia procedures simply cannot match.
3. Ultrasound: The Surgeon’s Third Eye
While ablation uses ultrasound for catheter placement, CHIVA uses it for hemodynamic architecture. We map the exact relationship between the Sural Nerve and the SSV before the first incision is made. This synergy between high-resolution imaging and surgical experience ensures that every ligation is strategic, purposeful, and—most importantly—safe.
At Dr. Smile Medical Group, our decade-long clinical data across five CHIVA centers reinforces the superior safety of this approach. Out of more than 2,000 limbs treated for Small Saphenous Vein (SSV) reflux, we recorded zero cases of permanent nerve damage. The only neurological incident was a single case of transient tibial nerve palsy, which resolved completely within a few hours. Retrospective analysis confirmed this was not surgical trauma, but a temporary nerve block caused by deep local anesthetic infiltration. This 0.05% transient event rate, compared to the much higher complication rates reported in thermal ablation literature, underscores the precision of the CHIVA protocol.


")
{kind=link}