
Lunch Talk delivered at Gleneagles Hospital Hong Kong
Good afternoon.
It is always a pleasure to stand in front of colleagues and speak about something that has occupied much of my professional life. Today, I would like to share not just a technique, but a different way of thinking about varicose vein treatment.
Why Do We Treat Varicose Veins?
Patients come to us for different reasons.
Some experience discomfort — heaviness, aching, fatigue.
Some are concerned about complications — ulcers, thrombosis.
And for many, it is also about confidence and quality of life.
All these reasons are valid.
But perhaps the more important question is not only why we treat,
but how we choose to treat.
Beyond Indications: What Matters Next?
In clinical practice, indications are only the beginning.
Patients are increasingly asking different questions:
- Is it safe?
- Will it work in the long term?
- How accessible is the treatment?
- And if recurrence happens — what can be done next?
These concerns often matter more than the procedure itself.
They reflect not only expectations, but also experience —
many patients we see today have already been treated before.
The Current Landscape — and Its Limitations
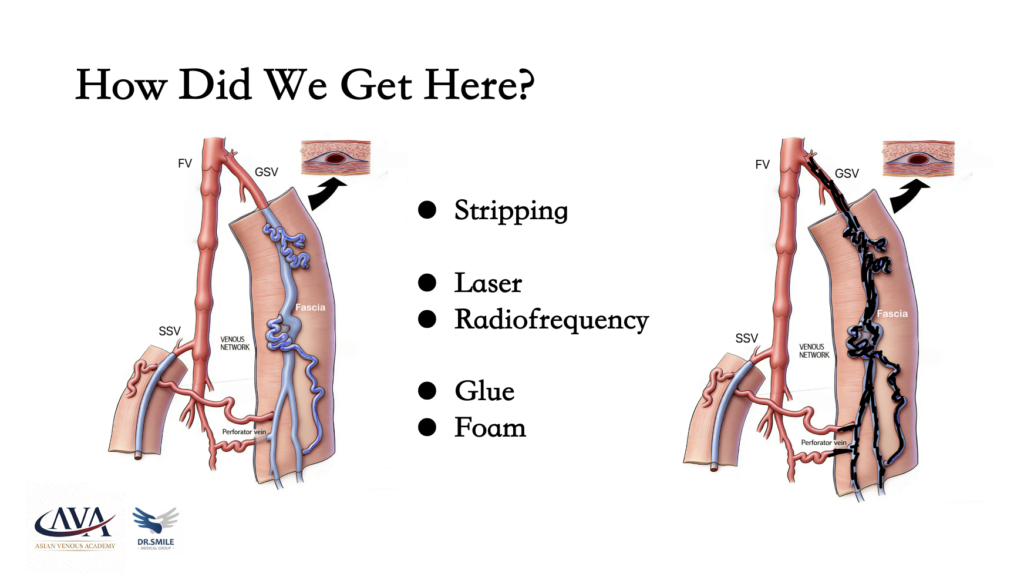
Over the past decades, we have seen significant evolution in treatment approaches.
We began with vein stripping.
Then came thermal ablation — laser and radiofrequency.
More recently, glue embolization has been introduced.
For smaller branches, we use sclerotherapy or phlebectomy.
Most of these approaches share a common focus:
the elimination of the saphenous trunk and visible varicosities.
And yet, despite these advances, we continue to face persistent challenges.
Recurrence remains a concern.
Complications still occur — nerve injury, hematoma, superficial or deep vein thrombosis.
And perhaps most importantly, long-term outcomes are not always satisfactory.
This leads us to a simple but important question:
Are we truly solving the problem?
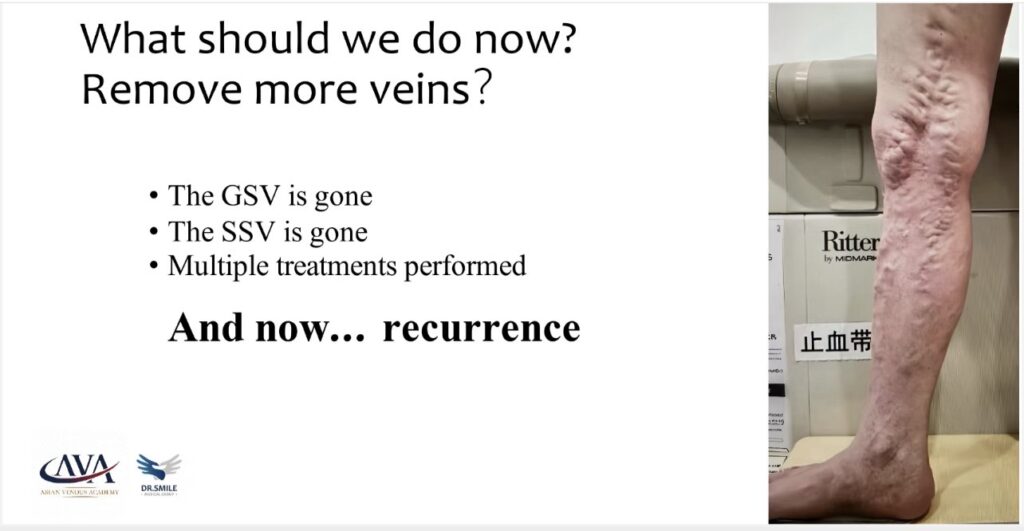
A Case That Changes the Question
Let me share a case.
A patient presented with extensive recurrence after multiple treatments:
great saphenous ablation, small saphenous stripping, and repeated sclerotherapy.
Despite all these interventions, the disease had returned.
At that moment, the question was no longer
“What else can we remove?”
Instead, we began to ask:
“What can we correct?”
This shift in perspective is where CHIVA begins.
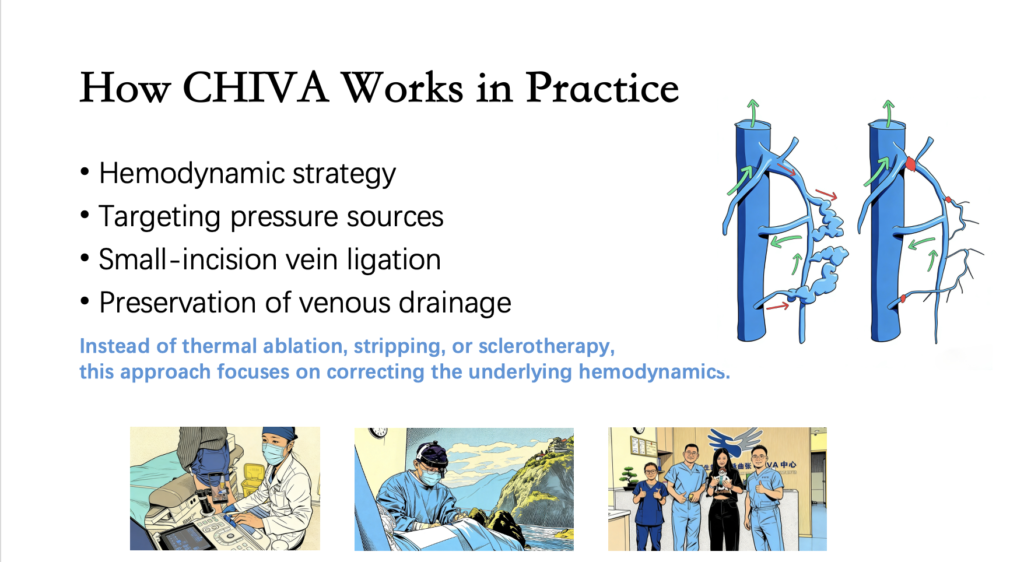
From Removal to Correction
CHIVA — Conservative Hemodynamic Treatment of Venous Insufficiency —
was introduced by Professor Claude Franceschi in 1988.
From the beginning, it was not about removing veins,
but about understanding and correcting flow.
Using duplex ultrasound, we identify the source of venous hypertension —
where the pressure originates.
We then target those specific points, interrupt pathological shunts,
and preserve the venous drainage pathways.
In practice, this often involves precise, office-based vein ligation
under local anesthesia.
We are not destroying the system.
We are restoring balance within it.

Understanding Pressure: A Simple Analogy
I often use a simple analogy.
Imagine a broken water pipe.
Water is spraying out under high pressure.
At first glance, the problem appears to be the leak.
But the real issue is the pressure behind it.
If we can identify the source of that pressure,
we do not need to remove the entire pipe.
We only need to close the right valve.
This is the essence of CHIVA.
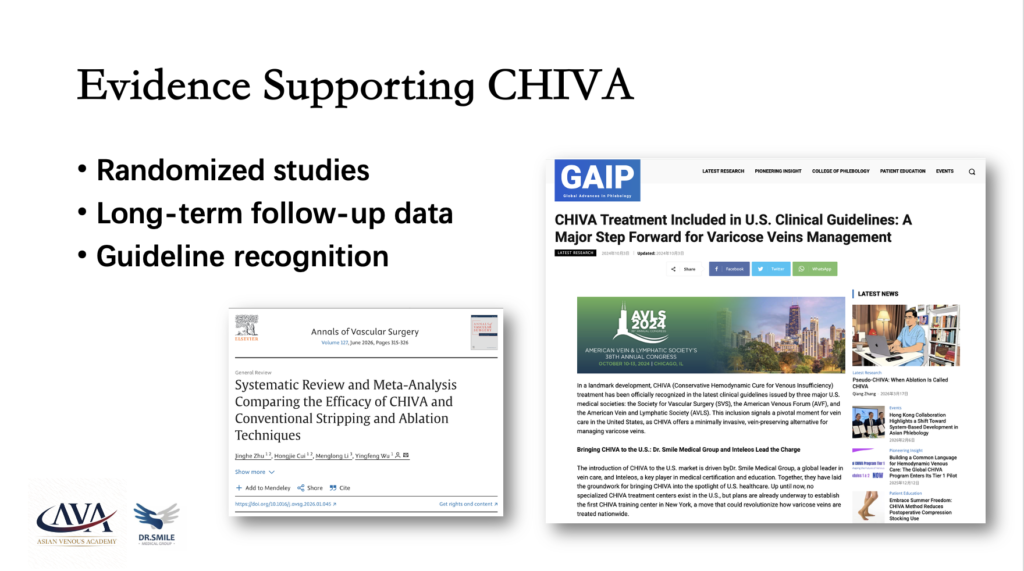
Evidence and Evolution
What was once considered a conceptual approach
has now been supported by growing evidence.
Randomized controlled trials and long-term follow-up studies
have demonstrated its effectiveness.
CHIVA has also been included in clinical guidelines
in multiple countries, including the United States.
This is no longer an isolated idea.
It is part of an evolving understanding of venous disease.
A Continuum of Care
Importantly, CHIVA is not just a procedure.
It is a system of care.
Before treatment, patients receive education and a detailed hemodynamic assessment.
During treatment, we focus on precise correction rather than extensive intervention.
After treatment, there is a period of adaptation — often around three months —
as the venous system reorganizes.
Beyond that, ongoing support remains essential.
In our centers, this includes continuous follow-up and, increasingly,
AI-assisted consultation available 24/7 in multiple languages.
Care does not end after the procedure.
What This Means for Patients
For patients, this approach offers several meaningful advantages:
- Treatment under local anesthesia
- Minimal risk of nerve injury
- Office-based procedures
- Faster return to daily life
- No requirement for compression stockings
And importantly:
Preservation of the venous system —
maintaining options for future cardiovascular or peripheral interventions.
In selected patients, recurrence may also be reduced.
The Challenge of Learning
At the same time, this approach is not easy.
It has a steep learning curve.
It requires a deep understanding of hemodynamics, not just the use of devices.
Each case is individualized — there is no standardized template.
And perhaps the most difficult part:
It requires us to rethink the disease itself.
Why This Matters
Despite these challenges, this work is worth doing.
Because ultimately, it is not about technique.
It is about patients.
One of our patients returned to running just two weeks after treatment.
Over time, he completed multiple marathons and even participated in triathlon events —
in his sixties.
These outcomes are not defined by veins alone.
They are defined by life.
A Different Way of Thinking
In the end, this is not just about how we treat varicose veins.
It is about how we understand them.
Not as a structural problem to be removed,
but as a hemodynamic imbalance to be corrected.
Closing
In the end, we are not just treating veins.
We are helping patients return to their lives.
To stay functional.
To stay active.
Thank you.



{kind=link}